



By Orlando Agrippa, founder and CEO, Sanius Health
Walk through any London commute at 8am and you’ll see the future of healthcare swinging off people’s wrists.
Thousands of tiny black screens flicker with heart rates, sleep scores, oxygen saturation, and stress metrics.
The population is quietly running a rolling clinical trial on itself while buying coffee, getting the Northern line, walking the dog. It’s not a niche behaviour anymore, it’s normal life.
And yet, inside the world’s largest publicly funded health system, we still behave as if patient-generated data is either a novelty or a liability.
That disconnect is bizarre, because the hardware problem is solved. It’s the cultural problem that is not.
The current gaps don’t stem from the technology at the heart of the matter suddenly getting better, but from a direction of travel that is no longer suitable.
Wearables have been explicitly positioned as part of the long-term NHS tech agenda, alongside the NHS App evolving into a more meaningful “front door”, and the Single Patient Record attempting to solve the fragmentation issue that makes modern care feel like a relay race with no baton.
Ultimately, the headlines and policy documents are all saying the same thing: the system wants this.
The problem is that wanting something and operationalising it are two very different sports.
Why Wearables Keep Getting Stuck in “Pilot Mode”
The NHS knows wearables can work. We’ve all seen the pockets of progress: virtual wards, post-operative recovery pathways, chronic disease monitoring, and oncology follow-up.
Where continuous signals have a clear purpose, you can make the case quickly and you can demonstrate value early on. And yet, the pattern repeats.
Wearables get deployed, outcomes look promising, and then the programme quietly stays local rather than becoming routine. It is rarely because the device didn’t perform, but more often because the system around it wasn’t designed to run at scale.
If you’ve worked in NHS transformation for any length of time, you’ll recognise the sequence: a tightly defined cohort, a time-boxed pilot, a motivated clinical team, early results, a poster, a write-up… and then reality hits.
Integration sits behind everything else.
Workforce capacity gets squeezed, and funding becomes uncertain, leaving behind a pilot that becomes a story people reference rather than a pathway people use.
Right now, most of the system still behaves like wearables are science fair projects. A ring here. A patch there. A 12-week pilot with a nice poster and a polite PDF. Then everyone moves on.
But the crux of the issue is that pilots do not scale. Plumbing scales. And while this might sound less exciting, this is ultimately the difference between a demo and a service.
Identifying the True Gap | Not an Issue of ‘Sensors’, But of the Translation Layer
From where we sit at Sanius Health, the idea that wearables are “emerging tech” feels out of date. They’re already ubiquitous.
The real gap is the translation layer between everyday life and a clinical pathway: how raw streams become something safe, useful, and actionable without turning clinical teams into full-time data interpreters, or shifting care into a constant state of alarm.
The NHS does not need shinier devices, but a way to turn millions of everyday signals into something a clinician can act on before lunch.
That translation layer is made up of the unglamorous questions that determine whether anything survives beyond the pilot:
- Who recruits patients and keeps them engaged when life presents challenges?
- How is consent managed so it’s remotely captured, portable, and robust?
- Where does the data land, and how does it integrate sensibly?
- What gets escalated, what gets ignored, and who owns the response?
- How do you avoid alert fatigue, false positives, and remote anxiety over time?
If you don’t answer those upfront, you end up with less of a wearable programme and something more akin to a wearable demonstration. This is something we learned the hard way.
Early on, we stopped asking, “Which device should we buy?” and started asking the questions that actually matter: “Where are the patients, what are they already willing to do, what devices work for them and their lifestyles, and what does long-term engagement look like?”
Once you start there, the rest changes.
We built around cohorts first, not the devices, ensuring we developed approaches based on real people and their experiences.
From initial consent to helping them stay active and engaged, this method has been contributing valuable longitudinal outcomes from home and in the community.
We then layered wearables in as a passive capture method that minimises the burden on patients while enriching what we could learn about their wellbeing, be these through bring-your-own-device routes where that made sense, or via lightweight clinical sensors when a pathway genuinely needed medical-grade and standardised capture.
That shift sounds simple, but it’s the difference between a programme you can publish and a programme you can repeat.
The effects are tangible when you get the foundations right.
Recruitment stops being a bottleneck because patients are already there and already engaged. Monitoring stops being episodic because you aren’t turning the tap on and off around appointments.
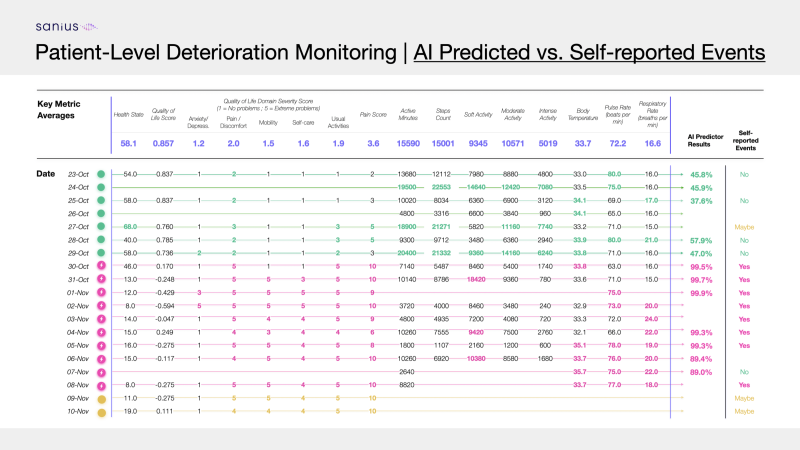
Clinicians stop drowning in raw numbers because what they see is change and pattern, not noise.
And commissioners stop asking why they’re funding “innovation” because you can show outcomes, pathway efficiency, and what it means for utilisation over time.
The wearable becomes invisible, which is exactly what you want.
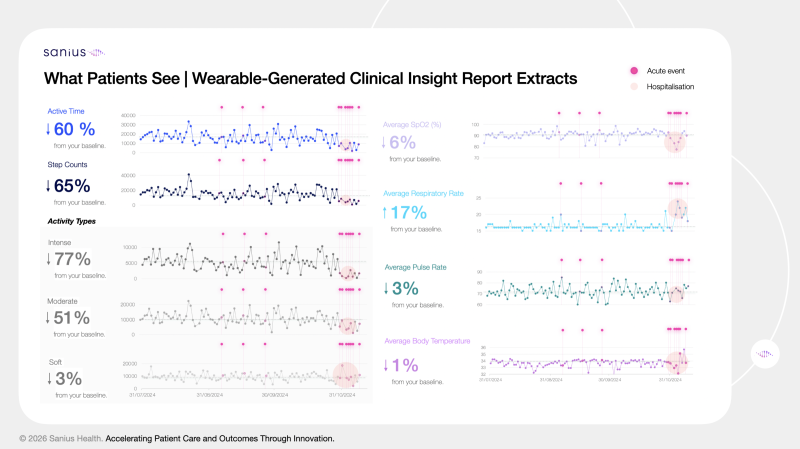
Critically, and at the heart of our work, patients get something that the NHS has historically struggled to offer at scale: visibility of their own health in between touchpoints, so they can act earlier and stay well at home, rather than waiting for things to deteriorate.
The Biggest Win is Patient Visibility, Not Clinician Surveillance
Wearables are often framed as a surveillance tool for clinicians. In practice, the biggest win is that they can be a self-management tool for patients.
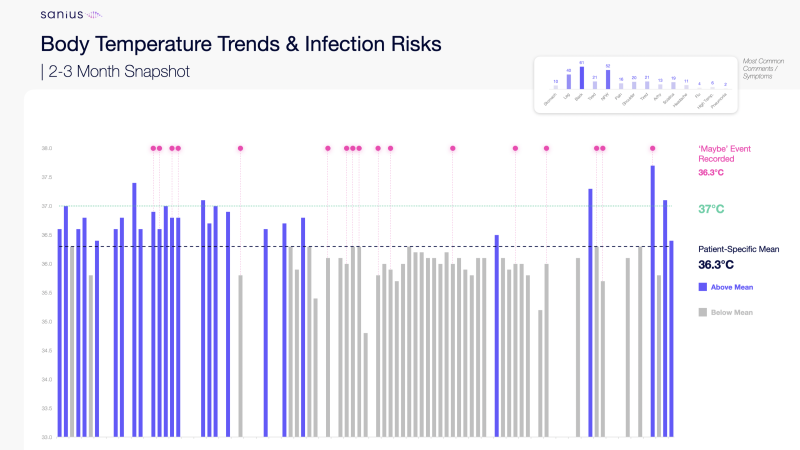
When someone can see their own baseline and what “normal for me” looks like, they make different choices earlier and at the first signs of change.
Visibility can support them in pacing themselves differently, prioritising rest, escalating sooner when something genuinely shifts. And perhaps most importantly, they feel less in the dark.
That kind of quiet empowerment is exactly what supports community care and staying well at home, without creating extra burden for clinical teams.
This is also why bring-your-own-device is unavoidable if the ambition is national scale.
Buying millions of medical-grade devices is a fantasy in a constrained system. But using the consumer devices half the population already owns is not.
The question is whether we build the governance, standards, and triage logic that make it safe to use, and whether we have the nerve to treat consumer wearables as part of a modern prevention and chronic care strategy, rather than a wellness toy we politely ignore.
Of course, there are genuine concerns that require addressing.
Data quality isn’t uniform across devices, liability isn’t trivial, and clinical accountability needs to be clear. But these aren’t reasons to stall, they are reasons to standardise.
What does “good enough” look like for each pathway? How do you summarise data so it’s interpretable quickly?
What triggers a nudge to the patient, what triggers non-clinical support, what triggers clinical review, and what triggers nothing at all?
If the pathway can’t answer those questions clearly, it won’t become business as usual.
The mythology around this space suggests you need futuristic command centres and million-pound procurements. In reality, you need something much less glamorous.
Identity. Consent. Integration. Standards. A clean data model. Someone responsible for watching the alerts. In other words, boring adult supervision.
Big tech figured this out years ago. Your phone already hoovers up steps, heart rate, sleep, location, and turns it into something intelligible before you have had your first coffee.
Healthcare can do the same. It just has to stop treating data like a legal liability first and a clinical asset second.
Across our programmes in haematology, cardiometabolic disease, oncology follow-up, rare conditions, and post-procedure recovery, we see the same pattern.
Creating an ecosystem comprising a patient-tailored ‘digital wallet’, integrated wearables, and wraparound support, our patient stories to date have reflected strong utility across the self-management journey.
“The digital wallet and wearable have completely changed how I manage my condition.
I feel much more in control now that I can see real-time data about my health, and it’s made discussions with my doctor so much easier.” – a Sanius Health member.
When you connect wearable signals to a real pathway, with named clinicians and defined actions, outcomes move fast. Fewer unnecessary visits. Earlier escalations. More confident discharges.
Patients feeling looked after without living in hospital car parks.
So, Where Are the Wearables?
They’re already everywhere. On wrists. In bedrooms. On kitchen tables charging next to the kettle.
The NHS doesn’t need to invent the future.
It needs to plug into the present, and then do what it does best when it’s at its most effective: take something that works, standardise it, and make it repeatable.
When all this happens, patients don’t just generate data – they gain visibility of their own health, the confidence to manage earlier, and a clearer path to staying well at home.
Indeed, the next decade won’t be won by whoever buys the most devices.
It will be won by whoever quietly builds the operating model underneath them, so wearables become boring, safe, routine, and genuinely useful.
Which is less headline friendly, admittedly, but far better for patients.
And if you have ever tried to explain to a board why your “transformational pilot” delivered exactly zero scale, you will know boring suddenly sounds very attractive.
Find out more about Sanius at saniushealth.com






